
My Shoulder “Itised”
The other day I was sitting on my couch watching a playoff game, and out of nowhere, my shoulder “itised.” I mean, I was just sitting there minding my business and BAM!

The “itis” hit me.
Nearly every other day, we get a call from a player or a parent or coach of a player with arm pain that has bee diagnosed as tendonitis.
The cycle they report is eerily familiar.
The player feels a little pain in their shoulder or elbow after throwing. It’s nothing major -just a pinch or a dull ache. They ice it, take some Motrin, Advil, or Tylenol, grease it up with Icy Hot and try to “throw through it.”
The pain persists and eventually gets worse.
They take a few days off, but when they start throwing, it hurts again.
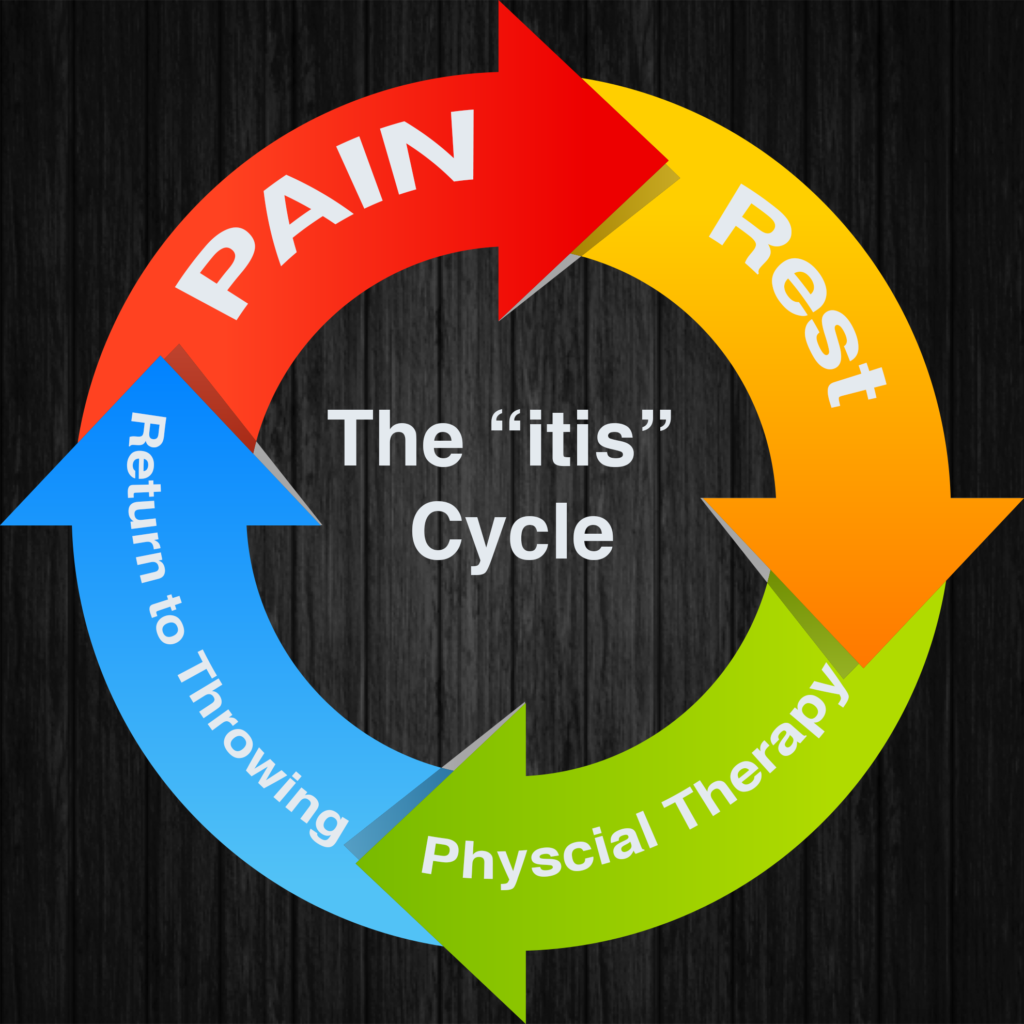
Finally, they visit their primary care doctor or orthopedist.
The doctor does some clinical tests and orders an x-ray, which nearly always comes back negative. The doctor tells them it’s probably tendonitis. He/she prescribes some heavier antiinflammatories or a Medrol Steroid Pack. Sometimes they even throw in a cortisone injection.
The doctor orders the athlete to take six weeks off from throwing and prescribes physical therapy.
The physical therapist performs an evaluation and determines that the player has weakness or “muscle imbalance” in his shoulder, scapula, forearm, and/or grip. The patient-athlete reports to the PT clinic 2-3 days a week for treatment that includes a five to ten minute warmup on the arm bike followed by theraband exercises for internal and external rotation, and flexion, scapular and rotator cuff “stability” exercises like rows, serratus pushups, and “throwers 10” exercises with 2-5 lb dumbbells. After about 20 30 minutes of exercise, ultrasound or electrical stimulation are applied to the painful area for 7-15 minutes, followed by 10 minutes of ice. During the ice treatment, the therapist documents the visit in the medical record and gives the athlete a set of exercises to do at home 2-3 times per day.
After 6 weeks, the athlete is discharged from PT with a return to throwing protocol that starts out with something like “25 throws from 45 feet at 50% effort.”
The athlete executes his plan and returns to play. And, the first time he ramps it up to full intensity, the pain returns. The player returns to the doctor or the PT, and the cycle begins again.
Please understand me clearly here. I am not disparaging anyone in the medical community. The process described is absolutely within the standard of care for the medical industry. I lived it every day for nearly 15 years. I prescribed and delivered all of those modalities and exercises and gave every player the same return to throwing protocol. Inevitably, the player would return with the same symptoms he had at discharge.
You may have heard me say this before, but when you tell me you have tendonitis, you might as well tell me you have a left eyebrow.
It doesn’t tell us anything.
Itises don’t just happen spontaneously.
If your arm “itises,” you have somehow allowed your connective tissue to be exposed to undue stress. And it’s very rarely one thing. It’s usually a combination of a lot of variables that merge to create an environment where pain or injury can occur.
We made a big leap forward in managing arm pain when we stopped looking for “diagnosis and cause” and began looking for “dysfunction and/or contributors.” We developed a thorough and meticulous evaluation process that ensures nothing slips through the cracks. And, we’ve become a world leader when it comes to solving arm pain for baseball players.
Eliminating arm pain begins with rejecting the flawed assumption that “you only have so many bullets in the gun.” Esteemed medical professionals, baseball coaches, and parents have been chasing pitch counts and innings limits for nearly 15 years, and the injuries keep mounting. One of the biggest obstacles to progress in the baseball training industry is the flawed assumption that heavy workload (overuse) is the primary “cause of injury.

In 2010 my friend, Ron Wolforth, came up with this list of the 6 types of contributors to subpar performance. As it turns out, the items on this list can also be significant contributors to arm pain. Listen, if you want to be a great thrower, you have to throw a lot. But, you have to get right with all the items on the list https://slot88ku.news/ to be able to throw enough to get good.
If you’re having arm pain, rest probably is not the answer. We need to get the core of the problem.
Give us a call at 866-787-4533 and let us evaluate you. We’ll design a training plan that will have your pain free and back in the game quickly. And we’ll ensure you solve the problem once and for all.
If arm pain is threatening to keep you off the field next season, you ABSOLUTELY MUST get it fixed. What happens if you rest all winter, then try to throw again and the pain comes back? You’d be in a heap of trouble.
Don’t let that happen to you. Get here.
Get started by calling, our CFO/COO Amy, at 866-787-4533.
We’ll see you at The ARMory.
About the Author:

Randy Sullivan, MPT, CSCS
CEO, Florida Baseball ARMory
Our founder and CEO, Randy Sullivan wears a bunch of hats: Physical Therapist, Baseball Instructor, Certified Strength & Conditioning Specialist, Paid Player Development Consultant to MLB teams, Public Speaker and of course an Author.